
The Intersection of Trauma and Intimacy: A Clinical Guide to Sex Therapy
By: Isaac Smith, MAT, LCSW, NTP
Licensed Clinical Social Worker | Founder, Whole Wellness Therapy | Sacramento & Fair Oaks, CA
Reading time: 12–14 minutes
Key Takeaways
Trauma lives in the body, not just the mind. The nervous system stores threatening experiences as physical responses — which is why intimacy can trigger fear, shutdown, or numbness even when you consciously feel safe with your partner.
Your reactions are not failures. Fight, flight, freeze, and fawn are automatic survival responses — not character flaws or signs you are incapable of closeness.
Sex therapy is talk therapy. There is no physical contact between therapist and client. It addresses the psychological and relational roots of intimacy difficulties, not just the physical symptoms.
Abuse and intimacy are frequently entangled. Around 80% of sexual assaults are committed by someone the survivor knows — meaning the body often cannot cleanly separate intimacy from threat without targeted therapeutic support.
Evidence-based modalities work. EMDR, somatic therapy, and DBT all have strong clinical research behind them for trauma and PTSD recovery — and each can be applied directly to intimacy healing.
Healing is possible for both individuals and couples. Whether you're working through your own history or trying to understand a partner's, trauma-informed therapy creates a path forward that neither of you has to navigate alone.
You don't need to have it all figured out before reaching out. The first step is a free 20-minute consultation — no commitment, no pressure, no requirement to have the words yet.
There's a version of this story that so many people carry quietly: you love your partner, or you want to. You feel safe in your relationship — or mostly safe. But the moment intimacy becomes physical, something shifts. A door closes. Your body goes somewhere your mind can't follow. Or you feel nothing at all, and then feel ashamed for feeling nothing.
If that resonates, I want you to hear this clearly: nothing is broken in you. What you're experiencing is a story about trauma — and about what happens when the past shows up uninvited in the most vulnerable spaces of the present.
In over fifteen years of clinical work — from DBT agencies to hospice organizations, from UC Davis Health to the practice I founded here at Whole Wellness — I've sat with a lot of people carrying exactly this. The experience is more common than most people know, and more treatable than most people hope.Sex therapy, particularly when it's trauma-informed, is one of the most effective pathways toward healing that intersection. This guide is for individuals and couples alike who suspect that past pain is shaping their present intimacy, and who want to understand both what's happening and what can actually help.
What Is Sex Therapy, and Who Is It For?
Sex therapy is a specialized form of psychotherapy that helps people address psychological, emotional, and relational factors affecting their sexual health and intimate relationships. Despite what the name might suggest, it is conducted entirely through talk therapy — there is no physical contact between therapist and client.
Sex therapists work with individuals and couples navigating a wide range of concerns, including:
Low or mismatched sexual desire
Difficulty with arousal, pleasure, or orgasm
Avoidance of intimacy or emotional shutdown during sex
Disconnection between partners around physical closeness
Recovery from sexual trauma or abuse
Pain during sex (vaginismus, dyspareunia)
Performance anxiety and pressure
Identity questions related to sexuality or gender
One of the most common — and most underrecognized — reasons people seek sex therapy is trauma. Not because they went looking for that connection, but because they finally found language for what's been happening in their body and their relationship for years.
If you're navigating intimacy challenges within a current relationship, oursex and intimacy counseling page covers more of what that work looks like for couples specifically.
How Trauma Disrupts Intimacy
To understand why trauma and intimacy collide so powerfully, it helps to understand what trauma actually does to the nervous system.
Trauma — whether it stems from childhood abuse, sexual assault, domestic violence, emotional neglect, or a pattern of relational harm — teaches the body one fundamental lesson: this was not safe. The nervous system stores that lesson not as a memory you can choose to recall or set aside, but as a physical, automatic response. Research published in the Harvard Review of Psychiatry established thattrauma is stored in somatic memory and expressed as changes in the biological stress response — meaning the body holds the history of what happened to it, and responds to present triggers accordingly. When something in the present environment echoes that past threat — a touch, a tone of voice, a specific moment of vulnerability — the brain activates its survival system before conscious thought can intervene.
This is not a character flaw. It is neurological adaptation. Part of what I find so important about the mind-body framework we use at Whole Wellness is that it takes this seriously — healing isn't only cognitive, it's somatic. Our post ontrauma and the brain goes deeper into the neuroscience of how this works — including why the body responds to perceived threat even when the conscious mind knows it's safe.
The Four Ways Trauma Shows Up During Sex
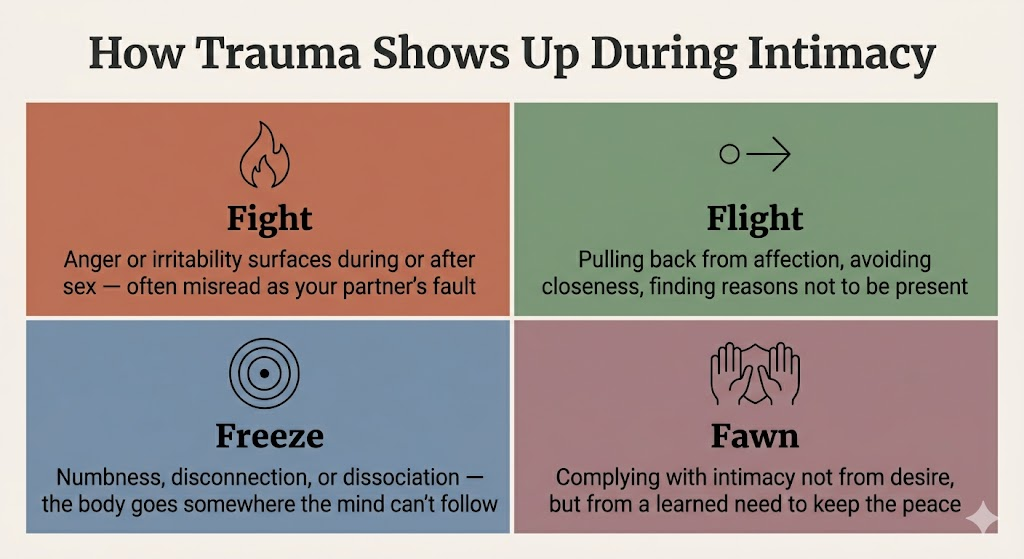
Trauma researchers describe the nervous system's threat responses using a framework sometimes called the 4 Fs:
Fight — irritability, anger, or emotional reactivity that surfaces during or after sexual intimacy. A partner may feel they've done something wrong when in reality the body is simply activating a defense it learned long ago.
Flight — avoidance. Pulling back from physical affection, finding reasons not to be present, gradually reducing intimacy without fully understanding why.
Freeze — the body goes still, numb, or disconnected. A person may feel like they're watching themselves from a distance, unable to feel pleasure or engage authentically. This is called dissociation, and it is extremely common among survivors of trauma, particularly sexual or physical abuse.Research has found that dissociative disorders are more commonly seen in victims of sexual abuse than in any other psychiatric population. Our post onwhat happens when your brain crashes describes this state — and why it's a protection response, not a personal failing.
Fawn — complying with intimacy not out of genuine desire, but out of a learned need to appease, avoid conflict, or feel safe. This pattern is closely tied topeople-pleasing behaviour and is especially common in survivors of relational abuse.
Each of these responses can look very different in a relationship. A partner observing avoidance or shutdown may interpret it as rejection, disinterest, or emotional distance. Without context — without a trauma-informed lens — couples can spend years in pain over a dynamic neither person fully understands. I've seen this play out across all kinds of relationships, and the relief that comes from simply naming what's happening is often the first real turning point.
The Role of Abuse in Intimacy Disruption
For individuals who have experienced abuse — whether in childhood, in a previous relationship, or in the current one — the impact on intimacy often runs especially deep. Abuse distorts some of the most foundational beliefs a person holds about their own body, their worth, and whether they are entitled to pleasure, boundaries, and safety.
Sexual violence is far more prevalent than most people realize.Over 50% of women and nearly 1 in 3 men report having experienced some form of sexual violence in their lifetime, according to the CDC. Research on childhood sexual abuse specifically shows thatprevalence ranges from 8–31% for girls and 3–17% for boys worldwide — and that adult survivors experience significantly higher rates of sexual dysfunction than non-abused individuals. Many of these survivors never connect their intimacy difficulties to their history of abuse.
Common themes that emerge in sex therapy with abuse survivors include:
Shame around the body — feeling that the body is dirty, damaged, or undeserving of care
Difficulty with boundaries — either struggle to assert them or an impulse to enforce them rigidly in ways that create distance
Confusion between sex and obligation — especially when abuse occurred within a relationship where intimacy was used as control
Hypervigilance during physical closeness — the body scanning for threat even when the mind knows the present situation is safe
Difficulty staying present — dissociation as a protective response that once served survival, but now interrupts genuine connection
RAINN notes thatearly sexual abuse can significantly disrupt a survivor's understanding and experience of intimacy, and that difficulty trustingvpartners, anxiety during intimacy, and intrusive memories are common and well-documented aftereffects — not signs of being broken.
Understanding howabusive relationships start and why people stay is often part of this work — because many survivors carry not just the wounds of what happened, but deep confusion about why it happened and what it says about them.
It's also worth naming something that often goes unacknowledged: trauma and intimacy difficulties don't only follow "obvious" abuse. Emotional neglect,abandonment trauma and anxious attachment, growing up in a home where affection was conditional or absent, religious shame around sexuality, a partner who frequently criticized your body — all of these experiences can leave lasting imprints on how intimacy feels and functions. In my work I also see how physical health factors — chronic stress, nutritional depletion, hormonal dysregulation — compound the picture in ways that are often overlooked in purely psychological approaches. True healing, in my view, addresses the whole person.
What Trauma-Informed Sex Therapy Actually Looks Like
Trauma-informed sex therapy doesn't begin with sex. It begins with safety.
Before any meaningful work around intimacy can happen, a therapist needs to help you — or you and your partner — establish a foundation of felt security: in the therapeutic relationship, in your own body, and in the relationship itself. This is what separates trauma-informed care from approaches that focus only on technique or behaviour change.
I'm not here to drive your bus. I'm here to help you read the map, understand the terrain, and figure out which route makes sense for where you're trying to go. At Whole Wellness Therapy, our approach tosex therapy is grounded in clinical modalities that have strong evidence behind them for trauma recovery. Here's what that work can look like in practice.
EMDR Therapy: Processing What the Body Has Stored
Eye Movement Desensitization and Reprocessing (EMDR) is one of the most well-researched trauma therapies available. It isrecommended as a first-line treatment for PTSD by the World Health Organization and is endorsed by the International Society for Traumatic Stress Studies and the National Institute for Health and Care Excellence. It works by helping the brain reprocess traumatic memories that have been stored in a fragmented, emotionally charged way — the kind of storage that makes them feel perpetually present rather than safely in the past.
Multiple randomized controlled trials have demonstrated its effectiveness. In one well-cited study,100% of single-trauma victims and 77% of multiple-trauma victims no longer met criteria for PTSD after a mean of six EMDR sessions. A 2024 scoping review foundpromising evidence for EMDR's efficacy specifically in treating trauma related to childhood sexual abuse, making it particularly relevant for the intersection of trauma and intimacy.
In the context of sex therapy,EMDR therapy can be particularly powerful because it targets the body-level responses that talking alone often can't reach. Many clients describe the experience as finally being able to hold a difficult memory without it flooding them — which over time changes how the nervous system responds during intimate moments.
EMDR does not require you to describe traumatic events in detail. It is structured, paced to your window of tolerance, and always led by your readiness. For survivors of sexual abuse or domestic violence, this quality of working with your nervous system rather than pushing through it is essential.
Somatic Therapy: Learning to Trust Your Body Again
The word somatic simply means "of the body." Somatic therapy works from the understanding that trauma is not only a psychological experience — it is a physical one. As research published in Frontiers in Neuroscience explains,trauma-related symptomology is grounded in nervous system dysregulation that cascades through physiological arousal, affect regulation, and higher-order functioning — the body holds the history of what happened to it, and healing often requires working at that level directly.
This is something I hold deeply in my own clinical philosophy. The mind-body connection isn't a wellness buzzword — it's neurologically real, and it matters enormously in trauma work. Arandomized controlled trial of Somatic Experiencing published in the Journal of Traumatic Stress found significant intervention effects for PTSD symptom severity and depression, with effect sizes ranging from 0.7 to 1.26 — making it one of the stronger body-based treatments studied to date.
In sex therapy, somatic approaches might involve:
Body awareness practices — learning to notice physical sensations without judgment, and to distinguish between anxiety and arousal, between tension and presence
Grounding techniques — practices that help the nervous system return from a state of activation to a state of felt safety
Titration — gradually and gently approaching intimacy in small increments, at a pace that the nervous system can tolerate and integrate
Breath work — using breath to shift out of the freeze or hypervigilance states that trauma activates
For couples, somatic work often includes structured exercises done at home — not sexual exercises, but exercises in non-pressured touch and presence — that help rebuild the felt sense of safety with another person's body.
Somatic therapy is especially valuable for survivors of abuse because it shifts the locus of healing back to the body itself. Rather than the body being a site of harm or a source of shame, it becomes a resource — a place of information, agency, and eventually, pleasure. This is core to what we mean byhealing after abuse and rebuilding yourself: not just recovering from what happened, but reclaiming who you are on the other side of it.
DBT: Building the Emotional Skills Intimacy Requires
Dialectical Behavior Therapy (DBT) is a skills-based therapeutic approach I've worked with extensively throughout my career — from my early years at DBT agencies to the integrative work I do today. Originally developed for people experiencing intense emotional dysregulation, it has proven remarkably effective in trauma contexts. A2024 meta-analysis published in the European Journal of Psychotraumatology found that DBT-based treatments for PTSD produced moderately beneficial effects on trauma symptom severity and depression — and in a landmark randomized clinical trial,DBT-PTSD outperformed Cognitive Processing Therapy for childhood abuse-related PTSD, with 58% of participants achieving symptomatic remission versus 41% in the comparison group.
In the context of sex therapy and trauma recovery,DBT therapy offers a practical toolkit for navigating the emotional landscape that intimacy stirs up.
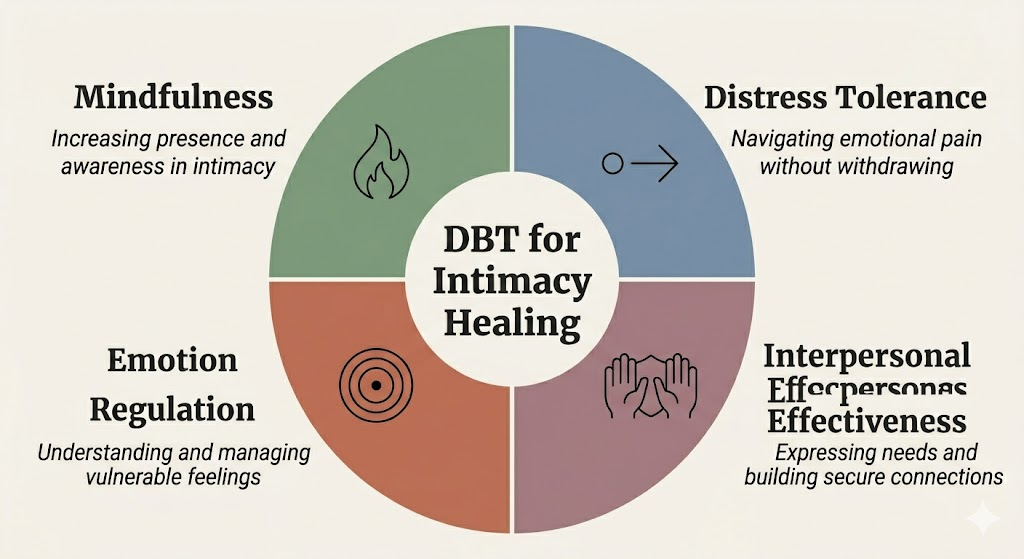
DBT's four core skill areas are directly relevant to healing trauma's impact on relationships:
Mindfulness — learning to stay present during intimate moments rather than dissociating or ruminating on past experiences
Distress tolerance — building the capacity to stay in emotionally difficult moments without escalating or shutting down entirely
Emotion regulation — developing the ability to understand and modulate the intense emotions — shame, fear, grief, anger — that trauma and intimacy can activate
Interpersonal effectiveness — communicating needs, limits, and desires clearly and directly, which is foundational to healthy sexual relationships
If you recognize yourself in these patterns — particularly the cycle of emotional intensity followed by shutdown or withdrawal — our post ondealing with emotional dysregulation may also be a useful read alongside therapy.
For individuals in recovery from abusive relationships, DBT is often particularly resonant because abusive dynamics frequently involved emotional chaos, boundary violations, and learned helplessness. DBT rebuilds exactly the capacities that those environments erode.
Other Therapeutic Approaches We May Draw On
Depending on your history and what you're working toward,trauma therapy at Whole Wellness may also incorporate:
Brainspotting — a body-based approach that locates and processes trauma stored in the nervous system through specific eye positions; closely related to EMDR and often used when verbal processing feels inaccessible
EFT (Emotionally Focused Therapy) — particularly valuable for couples, EFT works with the emotional attachment patterns that shape how partners connect and disconnect
ACT (Acceptance and Commitment Therapy) — helps clients develop psychological flexibility and move toward intimacy guided by values rather than avoidance of fear
Psychodynamic therapy — explores how early attachment experiences and relational history show up in current patterns of intimacy and connection
No single modality fits every person or situation. Part of what I value most about the integrative model we practice at Whole Wellness is working collaboratively to understand which approaches speak most directly to your nervous system and your history — and being willing to adapt as the work evolves.
A Note for Couples
If you're reading this as part of a couple — whether you're the partner carrying trauma, or the partner trying to understand and support — there are a few things worth saying directly.
For the partner who has experienced trauma or abuse:
Your responses are not failures. The shutdown, the distance, the difficulty being present — these are not signs that you are incapable of intimacy. They are signs that your nervous system is doing exactly what it learned to do to protect you. Healing is possible, and it does not require you to push through or perform your way to recovery. A trauma-informed sex therapist will always work at the pace your body can integrate.
For the supporting partner:
Your experience in this dynamic is real and valid too. Navigating a relationship where intimacy is complicated by trauma can leave you feeling rejected, confused, helpless, or guilty — sometimes all at once. Ourcouples counseling andrelationship therapy services create a space where both of those realities can exist simultaneously, where you can learn how to be a source of safety for your partner without losing yourself in the process.
Couples work in this space is not about diagnosing who is "the problem." It is about helping two people understand a shared dynamic that neither created intentionally, and build something different together. If the relationship context involves a history of harm, our post onthe psychology of abuse and healing offers additional framing that many couples find useful early in this process.
Common Questions About Sex Therapy for Trauma
Do I have to talk about my trauma in detail?
No. A good trauma-informed sex therapist will never push you to disclose more than you are ready to share. Approaches likeEMDR andbrainspotting are specifically designed to process traumatic material without requiring detailed verbal narration. You are always in control of the pace and depth of what you explore.
What if I'm not sure my experiences "count" as trauma?
Trauma is not defined by the severity of an event compared to someone else's experience. It is defined by the impact it has had on your nervous system and your life. If intimacy feels fraught, if you regularly shut down or disconnect during sex, if shame or fear are consistent features of your experience — these responses are worth taking seriously, regardless of what caused them.
Is sex therapy only for people who've experienced sexual abuse?
No. Sex therapy addresses any situation where psychological or relational factors are affecting sexual health and intimacy. Anxiety, depression, relational conflict, differing desire levels, past painful sexual experiences, body image concerns, grief — all of these can be meaningfully addressed in sex therapy, with or without a history of abuse or assault.
How long does sex therapy take?
This varies considerably depending on the person, the history, and the goals. Some people find significant relief in 10–16 sessions. Others, particularly those working with complex or long-standing trauma, engage in therapy over a longer period. What matters more than the timeline is that you are working at a pace that feels sustainable — not pushed. You can read more about what to expect on ourFAQ page.
Can sex therapy help if my partner won't come?
Yes. Individual sex therapy is highly effective. Understanding your own nervous system, your history, and your patterns — and developing new capacities to navigate intimacy — creates real change even when a partner isn't in the room. Often, that individual work shifts the relational dynamic meaningfully over time.
When Intimacy and Abuse Have Been Entangled
One of the most complex and painful dynamics that sex therapy addresses is the entanglement of intimacy and abuse within a relationship itself — past or present.
When someone has experienced abuse within a romantic partnership, the body often cannot cleanly separate "intimacy with this person" from the threat responses it learned during the abusive episodes. Even after a relationship ends, those associations can carry forward into new relationships, creating confusion and distress that is hard to explain to a new partner.
According to RAINN, approximately 80% of sexual assaults are committed by someone the survivor knows — a neighbor, family member, or romantic partner — which means the entanglement of intimacy and harm is not the exception for survivors; it is the statistical norm. Understanding the patterns ofhow abusive relationships start and why people stay is often the first step in making sense of this — not to assign blame, but to understand the psychological dynamics that kept you in something that hurt you.
If you're in the process of leaving or have recently left, our post onthe 3 things to do before leaving an abusive relationship and the broader guide onunderstanding and escaping abusive relationships are both worth reading alongside therapy.
For those navigating the aftermath, sex therapy often works in parallel with broadertrauma therapy: processing the experiences themselves, rebuilding a sense of safety and self-trust, and gradually re-approaching intimacy not as something that was taken or weaponized, but as something that can be reclaimed on your own terms.
Betrayal trauma — the specific wound that comes from being harmed by someone you trusted and depended on — deserves particular attention here. It affects not just how survivors feel about the person who hurt them, but how safe it feels to be close to anyone afterward. Sex therapy creates space to work through exactly that: the grief, the mistrust, and the slow rebuilding of the capacity for genuine intimacy.
This work is not linear, and it is rarely quick. But in my experience, it is some of the most meaningful work a person can do — the process of learning, through lived experience rather than just understanding, that your body belongs to you.
Taking the First Step
If you've read this far, something in this piece likely landed for you. Perhaps you've been carrying this quietly for a long time. Perhaps you've tried to explain it to a partner and run out of words. Perhaps you've wondered whether what you're experiencing is "enough" to seek help for.
It is. Reaching out when you're feeling this vulnerable isn't easy — but it's one of the bravest things you can do.
Our therapists inSacramento,Fair Oaks, andonline across California are trained in trauma-informed approaches including EMDR, somatic therapy, and DBT. We work with individuals and couples navigating the full complexity of trauma's impact on intimacy — with warmth, clinical depth, and a pace that respects your nervous system.
The first step is a free 20-minute consultation. There's no obligation, no pressure, and no requirement to have your story fully figured out before you reach out.
Schedule your free consultation →Learn more about our sex therapy services →Explore EMDR therapy at Whole Wellness →
If you or someone you know is in immediate crisis or danger, please visit ourcrisis resources page or contact the National Domestic Violence Hotline at 1-800-799-7233, or RAINN's National Sexual Assault Hotline at 1-800-656-4673.
About the Author
Isaac Smith, MAT, LCSW, NTPLicensed Clinical Social Worker | Founder & Executive Director, Whole Wellness Therapy
Isaac Smith is a licensed clinical social worker, functional nutritional therapy practitioner, and the founder of Whole Wellness Therapy. With over fifteen years of experience across diverse clinical settings — including DBT agencies, hospice organizations, and UC Davis Health, where he helped develop the substance use disorder treatment program and Collaborative Care model for chronic depression and anxiety — Isaac brings a grounded, integrative perspective to trauma and relational healing.
His approach is whole-person by design: drawing on his graduate training in clinical psychology (currently pursuing his doctorate at the Wright Institute), a master's in theology, and advanced certification in nutritional therapy, Isaac works at the intersection of mind, body, and spirit. He specializes in trauma, addiction, anxiety, and existential concerns, and brings particular depth to work with clients navigating the aftermath of relational abuse and complex PTSD.
California BBS License: LCSW75372
References & Further Reading
van der Kolk, B. A. (1994). The body keeps the score: Memory and the evolving psychobiology of posttraumatic stress. Harvard Review of Psychiatry.https://pubmed.ncbi.nlm.nih.gov/9384857/
Maxfield, L. et al. (2021). The role of EMDR therapy in medicine: Addressing psychological and physical symptoms stemming from adverse life experiences. The Permanente Journal.https://pmc.ncbi.nlm.nih.gov/articles/PMC3951033/
Montoya, C. N. et al. (2024). Knowledge about EMDR therapy and child sexual abuse: A scoping review. Trauma, Violence, & Abuse.https://pubmed.ncbi.nlm.nih.gov/39066607/
Brom, D. et al. (2017). Somatic experiencing for posttraumatic stress disorder: A randomized controlled outcome study. Journal of Traumatic Stress.https://pmc.ncbi.nlm.nih.gov/articles/PMC5518443/
Kearney, B. E., & Lanius, R. A. (2022). The brain-body disconnect: A somatic sensory basis for trauma-related disorders. Frontiers in Neuroscience.https://pmc.ncbi.nlm.nih.gov/articles/PMC9720153/
Bohus, M. et al. (2020). Dialectical behavior therapy for posttraumatic stress disorder compared with cognitive processing therapy in complex presentations of PTSD. JAMA Psychiatry.https://pmc.ncbi.nlm.nih.gov/articles/PMC7376475/
Vanderzee, K. L. et al. (2024). A systematic review and meta-analysis on the efficacy of DBT variants for PTSD. European Journal of Psychotraumatology.https://pmc.ncbi.nlm.nih.gov/articles/PMC11445934/
Gewirtz-Meydan, A. & Lassri, D. (2023). Between pleasure, guilt, and dissociation: How trauma unfolds in the sexuality of childhood sexual abuse survivors. Child Abuse & Neglect.https://www.sciencedirect.com/science/article/abs/pii/S014521342300176X
RAINN. (2024). For adult survivors of child sexual abuse.https://rainn.org/for-survivors-of-child-sexual-abuse/for-adult-survivors-of-child-sexual-abuse/
CDC. Sexual violence: Fast facts.https://www.cdc.gov/violenceprevention/sexualviolence/fastfact.html