
What Is the Neurobiology of Clinical Depression? An Integrative Approach
By Isaac Smith, MAT, LCSW, NTP | Licensed Clinical Social Worker, Nutritional Therapy Practitioner, and founder of Whole Wellness Therapy
You wake up exhausted after a full night of sleep. The things that used to bring you joy — a meal you love, time with people who matter, a project you care about — feel flat. Muted. Like watching a movie with the color turned off. Getting through the day takes everything you have, and somewhere underneath all of it, a voice is asking what's wrong with you for struggling this much.
I've sat with this experience hundreds of times across my career — in addiction treatment, in hospice, in homeless shelters, and in my private practice at Whole Wellness Therapy. And the first thing I want you to know is this: that voice asking "what's wrong with me?" is asking the wrong question. The better question is: what's happening in my brain?
Because depression isn't a character flaw. It isn't weakness. And understanding its biology — really understanding it — changes everything about how we approach getting better.
This article is written for educational purposes and is not a substitute for a professional mental health assessment. If you're experiencing symptoms of depression, please reach out to a qualified clinician. If you are in crisis, call or text 988.
Depression Is a Brain Condition, Not a Personal Failing
Clinical depression — formally known as Major Depressive Disorder (MDD) — is a condition in which the brain's structure, chemistry, and communication networks are functioning differently than they should. Not metaphorically. Measurably.
According to the Global Burden of Disease 2021 study, more than 332 million people worldwide are living with depression — and it accounts for the largest share of disability-adjusted life years of any mental health condition globally. Brain imaging research, genetic studies, and decades of clinical neuroscience have established that people with depression show real, observable differences in specific brain regions, altered activity in stress-response systems, and disrupted signaling between neurons. This isn't abstract — it's physical. And it helps explain why depression can feel so relentless, and why it almost never responds to simply "trying harder."
In my years of clinical work — including time developing and launching a Collaborative Care program at UC Davis Health specifically designed to treat chronic depression and anxiety — I've seen what happens when people finally understand the biology of what they're experiencing. The shame starts to lift. Self-compassion becomes possible. And the path forward becomes a lot clearer.
Understanding the neurobiology of depression doesn't erase the deeply personal nature of the experience. It adds a framework — one that replaces blame with curiosity, and hopelessness with a more honest question: what does my brain actually need to heal?
The Key Brain Systems Involved in Clinical Depression
Depression doesn't live in one place. It involves a network of brain regions and systems that interact in complex, sometimes reinforcing ways. Here's what the research shows us about the main players.
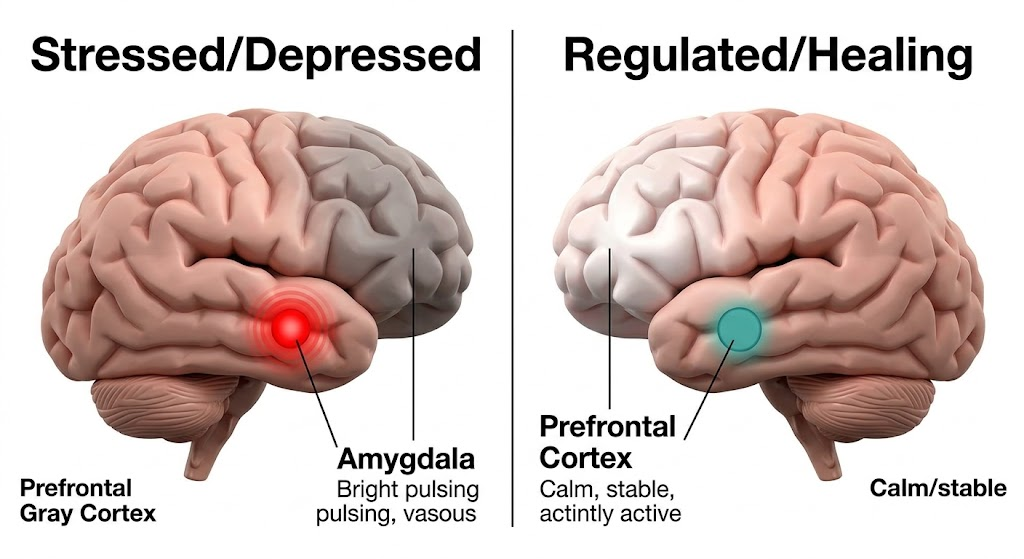
The Prefrontal Cortex
The prefrontal cortex (PFC) — the region just behind your forehead — handles the things we think of as being most essentially "us": decision-making, emotional regulation, planning, perspective-taking. Research published inNeuropsychopharmacology identifies the PFC as "one of the regions most consistently impaired in major depressive disorder," with both functional and structural changes visible on brain imaging. In depression, activity in the PFC tends to be significantly reduced, particularly in the areas responsible for modulating negative emotion and generating a sense of future possibility.
This is why you can't think your way out of depression. The very region responsible for stepping back, gaining perspective, and generating alternative views is running at reduced capacity. It's not a failure of willpower. It's a neurological reality — and one that responds to the right kind of treatment.
The Amygdala
The amygdala is the brain's threat-detection center, and in depression it tends to be chronically overactive. It fires more readily, holds on longer to negative experiences, and — with reduced prefrontal input to regulate it — doesn't get the "stand down" signal it needs.
The result is a nervous system biased toward threat, toward rumination, toward holding painful memories more vividly than joyful ones. This emotional reactivity can feel overwhelming and confusing — if you've ever wondered why your feelings seem to run the show even when you know better, theneuroscience of emotional dysregulation helps explain exactly what's happening underneath. Neurobiologically, that experience is not a character flaw. But it's also not permanent.
The Hippocampus
The hippocampus is central to memory formation and to regulating the body's stress response. A landmark meta-analysis in theAmerican Journal of Psychiatry confirmed that chronic depression is associated with reduced hippocampal volume — and, critically, that effective treatment can stop and even partially reverse this atrophy, likely by stimulating neurogenesis in the hippocampus.
This is one of the findings I return to most often in clinical work. The hippocampus is one of the brain regions most capable of neurogenesis — the growth of new neurons — throughout adult life. Effective treatment, including structured psychotherapy, consistent physical movement, and in some cases medication, has been shown to support hippocampal regeneration. The brain you have today is not necessarily the brain you'll have a year into good treatment.
Neurotransmitter Systems
You've probably heard the "chemical imbalance" explanation of depression — specifically, the idea that it's caused by low serotonin. This framing isn't entirely wrong, but it's significantly incomplete, and I'll come back to that in a moment. What the research actually shows is disruption across multiple neurotransmitter systems:
Serotonin regulates mood, sleep, appetite, and social behavior. Disruptions in serotonergic signaling contribute to many of depression's hallmark symptoms.
Dopamine drives motivation, reward-seeking, and the capacity to feel pleasure. Reduced dopamine activity is closely associated with anhedonia — that flat, colorless quality where nothing feels worth doing or enjoying.
Norepinephrine influences alertness, energy, and stress response. Its dysregulation contributes to the fatigue, brain fog, and physical heaviness that so many people with depression describe.
These systems are interconnected. Disruption in one ripples into the others — which is one reason why depression presents so differently from person to person, and why no single medication or approach works for everyone.
The HPA Axis and the Stress Response
The hypothalamic-pituitary-adrenal (HPA) axis is the body's central stress-response system — the machinery behind cortisol release. In people with depression, this system is frequently dysregulated, often stuck in a state of chronic overactivation.
Sustained elevated cortisol damages the hippocampus, disrupts sleep, impairs immune function, and amplifies the amygdala's sensitivity to threat. This creates a self-reinforcing loop that can be genuinely hard to interrupt from the inside: stress dysregulates the brain, the dysregulated brain becomes more vulnerable to stress, and around it goes. If you've ever felt like your brain justhits a wall and shuts down under pressure — that's the HPA axis and prefrontal cortex in conflict, and it has a name. Understanding the HPA axis also explains something I've observed consistently across every clinical setting I've worked in:depression and chronic stress don't just correlate. They actively maintain each other.
Why "Chemical Imbalance" Is Only Part of the Story
For decades, the dominant public explanation of depression was appealingly simple: your brain doesn't have enough serotonin. Take a medication that boosts it, feel better. This framing helped reduce stigma by offering a biological explanation, and for that it did some real good. But the science has moved considerably past it.
Here's what the evidence actually shows:
First — SSRIs increase serotonin availability within hours. If low serotonin were the whole story, they'd work in hours. For most people, meaningful relief takes weeks. And research consistently shows that a significant proportion of people with depression do not achieve adequate response from standard antidepressants — a 2024 networkmeta-analysis published in Neuropsychopharmacology reviewed 69 randomized controlled trials involving over 10,000 participants and found that treatment resistance remains a major clinical challenge. The "chemical imbalance" model simply doesn't account for this reality.
Neuroinflammation is emerging as a major piece of the puzzle. A growing body of research connects depression to elevated inflammatory markers in both the brain and body. According to a comprehensive review inFrontiers in Psychiatry, neuroinflammation affects roughly 1 in 4 people with depression and is associated with poor prognosis and treatment resistance. Inflammatory cytokines interfere with neurotransmitter metabolism, disrupt the HPA axis, and impair prefrontal function. For a subset of people — particularly those who haven't responded to conventional medication — inflammation may be a primary driver. This is one of the reasons I pursued advanced training in nutritional therapy: diet quality, gut health, and inflammatory load turn out to be meaningfully connected to depression risk and recovery in ways that most mental health training programs barely touch.
Disrupted neuroplasticity — the brain's capacity to change, adapt, and grow — is another central feature of depression. Chronic stress and neurochemical disruption effectively prune the brain's flexibility. One of the most consistent findings across treatment research is that effective interventions for depression — therapy, movement, sleep, certain medications — work in significant part by restoring neuroplasticity. The brain's capacity for change is not just a hopeful metaphor. It's a clinical mechanism.
Finally, the biopsychosocial model remains the most accurate framework we have. Biological factors (genetics, brain chemistry, inflammation, gut health) interact with psychological factors (thought patterns, trauma history, early attachment) and social factors (isolation, adverse life events, lack of meaningful connection). No single factor tells the whole story. And this is exactly why the most effective approaches to treating depression are integrative — addressing multiple levels at once rather than looking for a single fix. You can read more abouthow we put this model into practice in our clinical work at Whole Wellness Therapy.
I've worked with people in addiction treatment, in hospice, at homeless shelters, and in private practice. The people who make the most lasting progress in depression treatment are almost always the ones whose care addressed more than one dimension of the problem. That's not a coincidence. It's neurobiologically consistent.
What an Integrative Approach to Depression Treatment Looks Like
Understanding the neurobiology of depression shifts the clinical question from "what diagnosis do you have?" to "what does your specific brain and body need in order to heal?" These are very different questions, and they lead to very different treatment.
Here's how the main evidence-based approaches connect to the neurobiology we've covered.
How CBT Targets Cognitive Distortions in a Depressed Brain
Cognitive Behavioral Therapy (CBT) is one of the most extensively researched treatments for depression, and its effectiveness has a direct neurobiological explanation. Depression-driven thought patterns — all-or-nothing thinking, catastrophizing, relentless self-criticism — are partly the product of reduced prefrontal regulation and amygdala hyperactivity. They feel like the truth because, in the brain's current state, that's the clearest signal it can generate.
CBT works by systematically training the prefrontal cortex back online. A 2024 systematic review of task-based fMRI studies,published in NeuroImage: Clinical, found that CBT produces measurable changes in limbic reactivity and reward-processing activity in depressed patients — partially normalizing the neural patterns that drive negative cognitive bias. It's not just thinking differently. It's a different brain.
Learn more about our Cognitive Behavioral Therapy approach →
Motivational Interviewing and Building the Will to Heal
One of the more underappreciated challenges in treating depression is that depression itself undermines the motivation to engage in treatment. I'm a certified Motivational Interviewing (MI) practitioner, and I've come to think of MI as working at exactly the right level — not pushing people toward change, but helping them locate and connect with their own reasons for it.
This matters neurobiologically. Autonomous motivation — wanting change because it aligns with your own values, not because someone else thinks you should — activates different neural circuitry than external pressure. When people feel genuinely understood rather than managed, the therapeutic relationship itself becomes a restorative factor.
When Trauma and Depression Overlap
For many people, depression doesn't arrive in isolation. It develops in the context of unresolved trauma — adverse childhood experiences, relational wounds, chronic stress, profound loss. I've seen this across every clinical setting I've worked in, and it has a clear neurobiological basis: trauma dysregulates the HPA axis, alters amygdala reactivity, and can reshape hippocampal structure in ways that create enduring vulnerability to depression.
The relationship between trauma and the brain runs deep — and if you want to understand how that connection works at a neurological level, we've written abouthow trauma affects the brain in detail. When trauma is driving the depression, treating one without addressing the other is a bit like treating a wound without cleaning it first. The approaches that target trauma at a neurobiological level — includingEMDR and somatic therapies — often open doors that purely cognitive approaches cannot. You can also read more abouthow somatic therapy and EMDR work together when the body is holding what the mind hasn't been able to process.
Somatic and Body-Based Approaches
Because depression involves the body's stress-response systems — not just cognitive patterns — body-based approaches play a meaningful and often underutilized role in integrative treatment. Trauma-informed yoga, breathwork, and somatic work directly regulate the autonomic nervous system, helping bring a chronically activated stress response back toward balance.
Research on these approaches shows reductions in cortisol, improvements in HPA axis regulation, and increased prefrontal activity. This isn't alternative care. It's neurobiologically grounded treatment that addresses dimensions of depression that sitting and talking simply cannot reach. If you're curious about how this works in practice,trauma-informed yoga therapy is quite different from a standard yoga class — the distinction matters clinically, and we offer bothgroup and individual trauma-informed yoga sessions for clients who want to explore this approach.
Lifestyle Factors That Support Brain Recovery
This is where my training as a Nutritional Therapy Practitioner intersects directly with clinical depression treatment — and where I think conventional mental health care leaves the most value on the table.
The brain is not separate from the body. What happens in your gut, your immune system, your sleep, and your movement patterns is not background noise to your mental health. It's core to it.
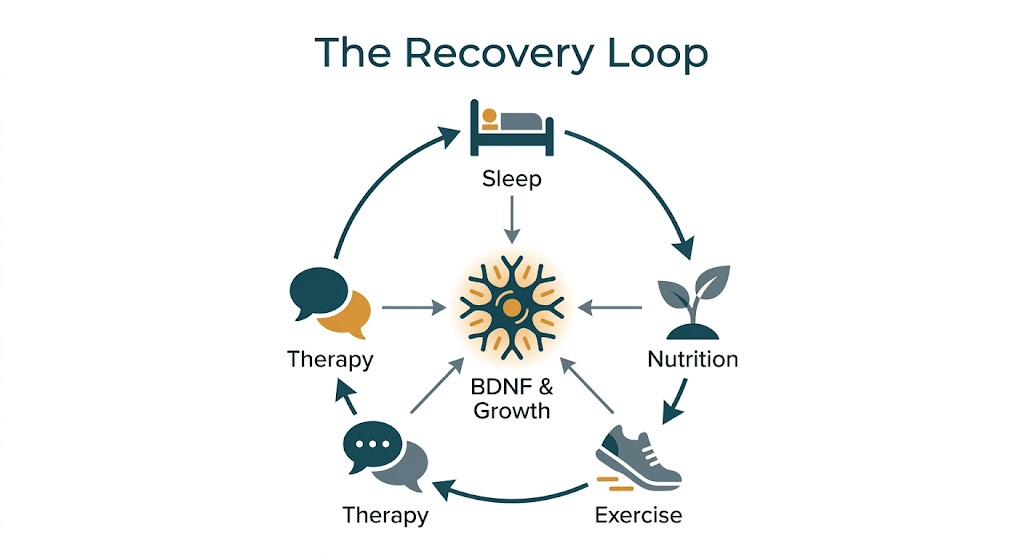
Sleep is when the brain consolidates learning, processes emotional memory, and clears metabolic waste. Chronic sleep disruption worsens HPA axis dysregulation and directly impairs hippocampal function. In my clinical experience, sleep is the lifestyle factor that produces the fastest measurable change when addressed well — and the one most people are willing to work on first.
Aerobic exercise is one of the most underutilized interventions in depression treatment. A meta-analysis covering 36 randomized controlled trials with 2,515 participants,published in Frontiers in Psychiatry, found that all exercise modalities significantly elevated BDNF (brain-derived neurotrophic factor — sometimes called "fertilizer for neurons") in people with depression. Exercise also promotes hippocampal neurogenesis, reduces inflammatory markers, and improves HPA axis regulation. The research is not subtle on this point.
Nutrition and gut health matter more than most mental health providers are trained to acknowledge. AsStanford Lifestyle Medicine notes, roughly 90% of the body's serotonin is produced in the gut — not the brain — through the activity of gut microbiota. Gut microbiome composition influences inflammatory load, neurotransmitter production, and stress reactivity. A diet that drives systemic inflammation is not a neutral background condition for someone with depression — it's an active headwind against recovery. We've explored this connection in depth in our piece ondepression and the gut, which is worth reading if you've ever suspected that what you eat affects how you feel mentally — because it does, and the science is increasingly clear on why.
Social connection is not a comfort — it's a biological necessity. Loneliness and social isolation activate the same neural threat-response systems as physical pain. Meaningful human connection, including the therapeutic relationship itself, is neurobiologically restorative. This is one reason I take the working relationship in therapy seriously — not as a mechanism for delivering techniques, but as a healing factor in its own right.
This is the Whole Wellness approach: treating you as a whole person — mind, body, and spirit — rather than a set of symptoms to be managed. Modern life is complicated, and your depression is happening in the context of all of it.
Frequently Asked Questions About Depression and the Brain
Can depression permanently change the brain?
Depression produces real, measurable changes in the brain — including reductions in hippocampal volume and altered prefrontal and amygdala activity. But the brain retains significant capacity for change throughout life. With effective, sustained treatment — including therapy, lifestyle changes, and when appropriate, medication — many of these changes are reversible. The hippocampus, in particular, can regenerate neurons. Recovery is a process, not a switch, but the neuroplasticity that makes it possible is real.
What does depression do to the prefrontal cortex?
In depression, the prefrontal cortex — responsible for emotional regulation, decision-making, and perspective-taking — tends to show reduced activity. This is why depression impairs concentration, amplifies negative thinking, and makes it genuinely difficult to "reason" your way out of a low mood. It's not a lack of effort. It's reduced neurological capacity in the very region responsible for the functions depression most disrupts. Effective psychotherapy, particularly CBT, has been shown to restore more typical prefrontal functioning over time.
Is depression just low serotonin?
No — and this oversimplification has caused a lot of confusion. Depression involves disruptions across multiple neurotransmitter systems (serotonin, dopamine, norepinephrine), the HPA axis stress response, inflammatory processes, and impaired neuroplasticity. Low serotonin activity is one component of a much more complex picture. This is one reason why personalized, multi-modal treatment tends to outperform any single intervention — because depression is rarely a single-system problem.
Can therapy actually change brain chemistry?
Yes, and this is one of the most important findings in modern neuroscience. Studies using brain imaging have shown that effective psychotherapy produces measurable changes in brain activity patterns, neurotransmitter function, and even hippocampal volume. Therapy doesn't just change how you think — it changes how your brain works. This is not a soft claim or a metaphor. It is a documented neurobiological effect, and it is one of the primary reasons evidence-based psychotherapy is considered a frontline treatment for depression, not a secondary option.
Am I depressed, or is this anxiety — or both?
This is one of the most common questions I hear, and it's a good one. Depression and anxiety frequently co-occur and share overlapping neurobiological mechanisms — particularly around the amygdala and HPA axis. They can look and feel similar from the inside, and distinguishing between them (or recognizing when both are present) matters for treatment. We've put together a detailed guide ontelling the difference between anxiety and depression that's worth reading if you're trying to make sense of what you're experiencing.
How do I know when it's time to reach out for professional help?
If depressive symptoms — persistent low mood, loss of interest, fatigue, sleep changes, difficulty concentrating, feelings of worthlessness or hopelessness — have lasted more than two weeks and are getting in the way of your daily life, professional support is appropriate. You don't need to be in crisis to deserve care. Earlier intervention tends to produce better outcomes, and a skilled therapist can conduct a proper assessment and work with you to develop an approach tailored to your specific situation — not a generic protocol, but something built around you.
You Don't Have to Navigate This Alone
So it goes with the human condition — messy, complicated, and more resilient than we give it credit for. Depression is one of the most common and most treatable mental health conditions in the world. Understanding its neurobiological basis doesn't make the experience any less real or any less hard. But it does offer something genuinely useful: a framework for healing that isn't rooted in self-blame.
Your brain can change. The right support makes that change more likely, more durable, and considerably less lonely. I've watched this happen more times than I can count — in addiction treatment, in grief work, in the quiet rooms of a hospice unit, and in the everyday courage it takes to walk into a therapist's office for the first time.
If you're ready to take that step, we make it easy to get started. Our Care Specialist Aeriana will answer your questions and match you with the therapist whose approach, expertise, and personality are the right fit for your particular adventure through this life.
Start with a free 20-minute consultation — no obligation, just a real conversation.
We offer in-person therapy in Sacramento (Midtown), Fair Oaks, and San Diego, as well asonline therapy for anyone in California.
About the Author
Isaac Smith, MAT, LCSW, NTP is a Licensed Clinical Social Worker, Nutritional Therapy Practitioner, and the founder and Executive Director of Whole Wellness Therapy. He holds graduate degrees in social work (USC), psychology (The Wright Institute), and theology (Fuller Theological Seminary), and is currently completing his doctorate in clinical psychology. Isaac previously developed and launched the Collaborative Care program at UC Davis Health, specializing in chronic depression and anxiety treatment. He has worked across addiction treatment, hospice, DBT-specialized agencies, and community mental health, and has been working with youth, adults, and families since 2007. He is certified in Problem Solving Therapy and Motivational Interviewing.
California Board of Behavioral Sciences License Number: LCSW75372
This article is intended for informational and educational purposes only. It does not constitute medical advice, a clinical diagnosis, or a recommendation for any specific treatment. If you are experiencing a mental health crisis, please contact the 988 Suicide & Crisis Lifeline by calling or texting 988.